Most cases of leprosy result from infection with Mycobacterium leprae. The M. leprae bacillus was identified by a Norwegian doctor, G.A. Hansen, in 1873. In 2008, scientists discovered a second leprosy-causing bacillus, which they named Mycobacterium lepromatosis.
Leprosy is thought to be transmitted through the air via droplets from the nose and mouth during close and frequent contact with untreated individuals.
95% of people have sufficient natural immunity and will not develop leprosy if exposed.
Not hereditary.
Not a curse nor a divine punishment.
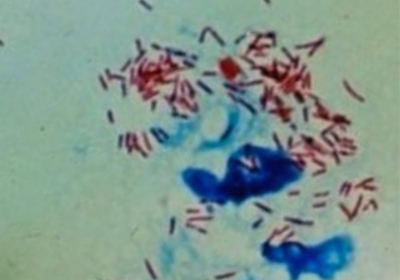
Mycobacterium leprae as seen through a microscope. Image courtesy of Infectious Disease Surveillance Center (IDSC), Japan.
Symptoms
The first outward sign of leprosy is the appearance of numb, discolored patches on the skin.
Enlarged nerves can also be a sign of the disease.
If leprosy progresses unchecked, it leads to loss of sensation in the limbs, paralyzed muscles, ulcers, injuries, and secondary infections.
A New Atlas of Leprosy, a pictorial manual published by Sasakawa Health Foundation to assist frontline health workers and volunteers in the detection, diagnosis, and treatment of leprosy.
Cure
Leprosy is treated with multidrug therapy (MDT) composed of an orally administered regimen of three drugs—rifampicin, dapsone, and clofazimine—taken for 6 to 12 months.
MDT is provided free of charge throughout the world via the World Health Organization (WHO).
After the first dose of MDT, a patient is no longer infectious.
Multidrug therapy is provided in calendar blister packs.
Prevention
There is no WHO-recommended vaccine for leprosy, but research is underway.
WHO guidelines recommend the use of single-dose rifampicin as a preventive treatment for adults and children (aged above 2 years) who are in regular contact with leprosy patients.
The Bacillus Calmette-Guérin (BCG) vaccine, used primarily against tuberculosis (TB), has been shown to reduce the risk of leprosy.
Diagnosis by a coordinator for the state health department’s leprosy program (Mato Grosso, Brazil, 2015).